Cervical cancer is the fourth most common cancer in women globally. In 2020, there were an estimated 604,000 new cases and 342,000 deaths. The American Cancer Society estimates that the USA in 2022:
- About 14,100 new cases of invasive cervical cancer will be diagnosed.
- About 4,280 women will die from cervical cancer.
Quick Navigation
What is Cervical Cancer Screening?
This refers to the tests done to find changes in the cervix cells that could lead to cancer.
Screening aims to identify precancerous lesions that could lead to invasive disease. Identification of precancerous lesions saves lives and reduces the disease burden as they can be treated far easier than what would entail for a full-blown malignancy.
Cervical screening includes:
- Cervical cytology with Pap (Papanicolaou) smear
- Testing for High-Risk Human Papilloma Virus (hrHPV)
- Co-test
- Visual Inspection with Acetic Acid (VIA)
- Visual Inspection with Lugol’s Iodine (VILI)
1. Cervical cytology (Pap test or Pap smear)
Samples are taken from the cervix in the outpatient department and sent for study under the microscope. Pap smear detects precancerous or abnormal cell changes that might undergo cancerous changes if not treated.
2. Testing for High-Risk Human Papilloma Virus (hrHPV)
This test is done on a sample of cells removed from the cervix, often at the same time taken for a Pap smear. This sample is tested for Human Papilloma Virus (HPV) strains that are most commonly linked to cervical cancer.
*hrHPV: More than 200 types of HPV have been identified, with ~30 affecting the genital tract. hrHPV refers to High-Risk HPV strains that can induce malignant tumors even at low levels.
3. Co-test
Combined Pap test and hrHPV testing.
4. Visual Inspection with Acetic Acid (VIA)
This is a direct inspection of the cervix after the application of diluted acetic acid, which turns the cancerous areas white.
5. Visual Inspection with Lugol’s Iodine (VILI)
Lugol’s Iodine reacts with glycogen resulting in brown or black coloration. Normal cells contain glycogen, and when in contact with Lugol’s iodine, it becomes black, whereas precancerous lesions and cancer have little or no glycogen, thus turning yellow after Lugol application.
* Pap smear, hrHPV, and a combination are what is generally practiced in resource-rich settings.
*VIA and VILI are often combined with resection of the affected area in the same sitting and are often a method of choice in resource-poor settings.
Home Self-testing Cervical Cancer Screening
HPV self-sampling can greatly improve access to cervical cancer screening as it is convenient, less embarrassing, relieves the anxiety of a doctor’s visit, lower cost, and less discomfort. There is also an increasing body of evidence to support its efficacy and utility. However, this is not FDA approved, is still in investigational stages, and thus, cannot be recommended yet as a replacement for more established methods.
Click here to learn more about home self-testing for cervical cancer screening and commercially available kits.
Why is it essential?
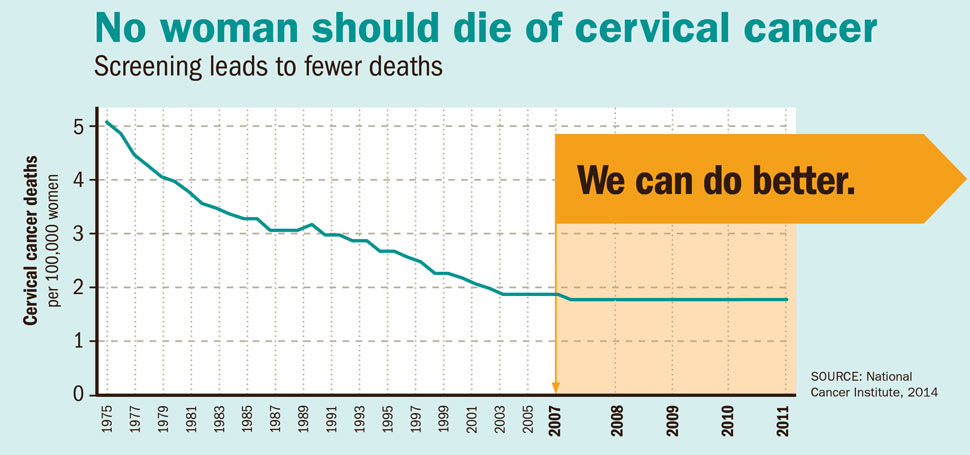
In the USA, around 14,000 women are diagnosed, and 4000 die yearly. Screening leads to fewer deaths.
Studies have shown that screening reduces the incidence of cervical cancer by 50 to 60%
Over 95% of the burden of cervical cancer is potentially avoidable by good screening programs and vaccination against HPV16 and 18 – the latter being the causal agent for up to 70% of cervical cancer.
Screening recommendations
The USPSTF (US Preventive Services Task Force) in 2018 updated its recommendations for cervical cancer screening. These recommendations have been endorsed by The American College of Obstetricians and Gynecologists (ACOG), The American Society for Colposcopy & Cervical Pathology (ASCCP), and the Society of Gynecologic Oncology (SGO).
*These recommendations are not a blanket application for the whole population. For exceptions, read the Special Cases section of this blog.
| Younger than 21 years | Screening not needed | |
| 21 to 29 years | Pap smear alone every 3 years Or HPV testing alone if 25 to 29 years, but Pap test is preferred. | |
| 30 to 65 years | Any one of the following: Pap test alone every 3 years Or HPV test alone every 5 years Or Pap test + HPV test every 5 years | |
| Older than 65 years | No screening needed if: No past history of cervical changes + Within the past 10 years: 3 negative Pap tests in a row Or 2 negative HPV tests in a row Or 2 negative co-tests in a row (The most recent Pap test should have been done in the past 3 years and the HPV or the co-tests within the past 5 years) |
* As the prevalence of HPV vaccination is increasing, there have been recommendations to change the screening initiation age from 21 to 25, but due to disparity on the grounds of race, ethnicity, region, and socioeconomic status, that affects the prevalence of HPV vaccination and access to healthcare, the age of 21 is still being adhered to.
Special Cases (Vaccination, Pregnancy, HIV, Surgery)
*The screening tests recommendations here refer to cytology, hrHPV, and co-test.
I have had an HPV vaccination. Do I still need to undergo regular screening?
You will still need to undergo age-specific screening because:
- The vaccine does not protect against all strains of HPV.
- You might have been exposed to HPV before you were vaccinated, and the vaccine does not treat the infection you already have.
- Vaccination does not guarantee 100% immunity against a disease.
I am pregnant and my screening is due. Should I?
Cervical Screening Tests have not been linked to increased miscarriage rates. Furthermore, once the baby is born, it might be harder for you to take time out. If you undergo screening after pregnancy, ideally wait for 3 months post-delivery as the cervical cells may still be inflamed. Contact your gynecologist for more details on this.
I have had a hysterectomy. Do I still need to be screened?
- had a hysterectomy as part of treatment for high-grade cervical abnormalities or cervical cancer,
- had a previous high-grade cervical abnormality,
- had cervical abnormalities detected during hysterectomy.
I am HIV positive. How does that change my screening schedule?
Pap smear is the primary mode of screening
Ages 21 to 29 should have a Pap test at the initial time of HIV diagnosis.
If normal, the next testing is at 12 months.
If 3 consecutive Pap smears are normal, then follow-up Pap tests are recommended every 3 years.
For more information on this topic, click here to go to the CDC website.
Takeaway
- It is estimated that the USA in 2022 will have ~14,100 new cases of invasive cervical cancer and ~4,280 women will die from cervical cancer.
- Over 95% of the burden of cervical cancer is potentially avoidable by good screening programs and vaccination.
- Cytology and hrHPV tests are used in resource-rich communities. Resource-poor communities often have to rely on VIA & VILI.
- There are standard screening recommendations that are modified in special circumstances like pregnancy, HIV positive, and those with history of hysterectomy.
